Introduction
Post-medieval England (1700-1850) demonstrated a vast amount of change in society; the urbanisation of cities that came with the Industrial Revolution (1760-1840) altered the landscape and health of the populations considerably. Although arguably a noticeable change was the rise of middle and upper classes, which created a larger divergence between the poor and the wealthy (Mays et al. 2008, 86).
The conditions for the working classes tend to be reflected upon with negative connotations; for the urban disadvantaged, work was often in industrialised factories; the hours were long, and the workers were only allowed rest for one day a week (Gowland 2018, 153). Life for the rural poor, in contrast, is suggested to have had a relatively improved quality of life attributed to the lack of pollution and overcrowding, although laborious work was equally as intense for both sexes and all ages as urban life (Gowland et al. 2018, 27). The middle and upper classes enjoyed a more leisurely life, with the only indicators of trauma often being reflective of social sport, rather than laborious work (Cunningham 2016, 12).
The significance of investigating post-medieval burials is that the identity of the individuals can often be ascertained with reference to direct historical accounts and grave-markers, which allows a direct comparison of social status and health, as the status can be inferred more directly. Evidently, the transition to urbanisation and industrialisation is likely to have affected the health and diet of different class populations. Three cemeteries from urban London of equal size will be assessed; two of which hold a more affluent status (Chelsea Old Church and St Marylebone), while the third example (St Brides Lower) represents the lower classes. To explore the extent that social status was an exclusive factor in influencing health and diet, a fourth cemetery from a rural environment (Fewston) will be discussed. See Figure 1 for a map of the context.
![Figure 1: Map of cemeteries studied in this essay. Porter, C, "Map of Cemeteries Used" [JPG map], Scale 1:100000, GB Overview [ geospatial data], Updated: 2019, Ordnance Survey (GB), Using: EDINA Digimap Ordnance Survey Service, <http://digimap.edina.ac.uk/>, Created: October 2019.](/sites/theposthole.org/files/styles/medium/public/articles/454/fig%202.png?itok=A2Y37WzD)
Health and Diet
Health and diet are not mutually exclusive; it is widely asserted that a poor diet can result in a diminished immune system which will lower the chances of successfully combatting infections and diseases, and contributes to the development of chronic skeletal defects (Roberts and Manchester 2010, 223). This section will explore how far social affiliation negatively impacted the health and diet of individuals from contrasting social classes within urban and rural England by assessing the skeletal data for four possible status-impacted conditions.
Working Class
The consequences of being born into a poor socio-economic family were rooted during this period. Women and children were more likely to be involved in non-domestic labour, which comprised of long hours away from home, often in factories with little exposure to sunlight (Roberts and Manchester 2010, 238). Taking women out of the household and inserting them into manual work also had a negative effect on familial health pertaining to diet; commercially produced meals were made available but were deficient in essential vitamins (Horrell and Oxley 2012a, 1359).
The human body cannot synthesise itamins alone, therefore, skeletal and dental development must be maintained by a balanced diet (Fitzpatrick et al. 2012, 395). Consequential to the health of poorer households, food consumption was largely based on regional availability and household earnings; a consequence of bad harvests lead to price inflation, lack of time and common land to grow fresh produce, in addition to the decline of livestock due to the high prices of feeds (Horrell and Oxley 2012a, 1359-1364).
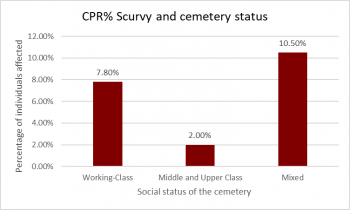
Vitamin C is found in fresh fruit, vegetables, and marine fish. Chronic lack of Vitamin C is more prevalent in the poorer socio-economic individuals within the sample (Figure 2). This dietary deficiency manifests in cases of scurvy, which is caused by a prolonged Vitamin C depletion and is identified skeletally by the presence of ossification and porosity (Figure 3) (Newman and Gowland 2016, 220).

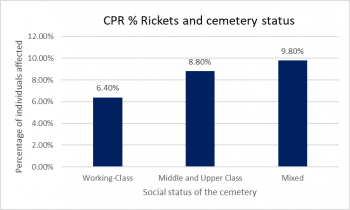
In contrast, Vitamin D deficiency is predominantly caused by a lack of exposure to ultraviolet rays, which is essential for the mineralisation of osteoid and cartilage to maintain bone density (Roberts and Manchester 2010, 237). In children, a sufficient lack of Vitamin D during the vulnerable stages of development, can disrupt bone mineralisation in the growth plates and lead to rickets, and subsequent deformation of the weight-bearing limbs (Roberts and Manchester 2010, 237).
Children are more susceptible to developing rickets due to their weakened immune system and the physiological demands of skeletal development; whereas adults are more likely to develop osteomalacia, which occurs as a result of delayed mineralisation of osteoid in cortical and spongy bone (Newman and Gowland 2016, 220; Roberts and Manchester 2010, 237). While rickets tends to be a condition of infancy (Mays et al. 2006, 362), it can be argued that the post-medieval children often developed rickets during later childhood years (Figure 4 and 5). The direct influence can be attributed to the reliance of many families on the wages of their young children; with the work comprising of long hours in factories with sparse exposure to sunlight, in addition to non-nutritious meals and the adverse mental state caused by poor working conditions (Roberts and Manchester 2010, 238).

Middle and Upper Classes
It is assumed that the more affluent members of society would display less evidence for dietary deficiencies, and would instead show a positive correlation for dietary excess due to their accessibility of expensive food sources (Roberts and Cox 2003, 310). However, both the lower and higher-class individuals from this sample shared high prevalence rates for Vitamin D deficiency rickets.
It can be suggested that the individuals affected from the high-status cemeteries were less likely to develop rickets from deplorable working conditions, and were more likely to develop rickets at a younger age attributed to contemporary parenting practices (Roberts and Manchester 2010, 239). For high-class women, breastfeeding declined as shop-bought formula was readily available, albeit deficient in vitamins and proteins (Roberts and Manchester 2010, 239; Stevens et al. 2009, 34-37). Therefore, although poorer children developed rickets as a result of poverty, the practices of the socially elite did not always constitute a healthier society.
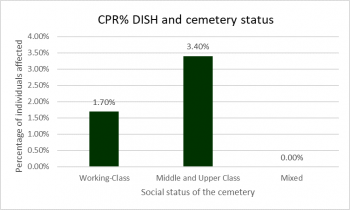
One of the effects of urbanisation in England was the efficient transport infrastructure, which enabled food to be shipped around the country for those who could afford it (Bleasdale et al. 2019, 6161). As a high calorific intake for this period is representative of wealth and therefore high-status, a direct consequence of a high-status lifestyle on health can be identified skeletally by the presence of diffuse idiopathic skeletal hyperostosis (DISH). The direct aetiology of DISH is complex, although its predominant associations have been linked to obesity and diabetes mellitus (Roberts and Cox 2003, 311; Bombak 2012). DISH manifests on the spine and is identified by new bone formation in a candle-wax like appearance on the right side of the vertebra, causing fusion (Bombak 2012; Roberts 2018).
In this sample, the higher-class individuals displayed a prevalence rate of DISH which was double the individuals affected from the lower-class cemetery (Figure 6 and 7). Therefore, the increasing range of food resources that were available to the higher classes, particularly animal proteins, can be suggested to have negatively impacted health.

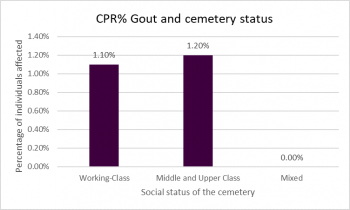
A final example of the consequences of an excessive diet, which is often associated with high status, is gout. Gout is a form of inflammatory arthritis, which is caused largely by prolonged consumption of purine-rich foods and alcohol (Buckley 2011, 110; Howard et al. 2016, 2). A key marker of gout skeletally is erosive lesions on the joint surfaces (Figure 8).
Contradictory to expectations, the prevalence rates for the presence of gout were relatively low in this sample at 1.2% (6/502) (Figure 9); although this could be attributed to a bias in regional availability of food resources.

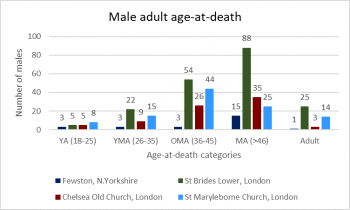
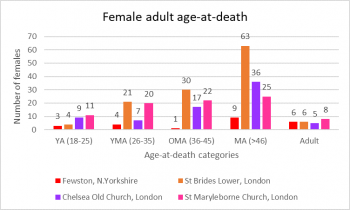
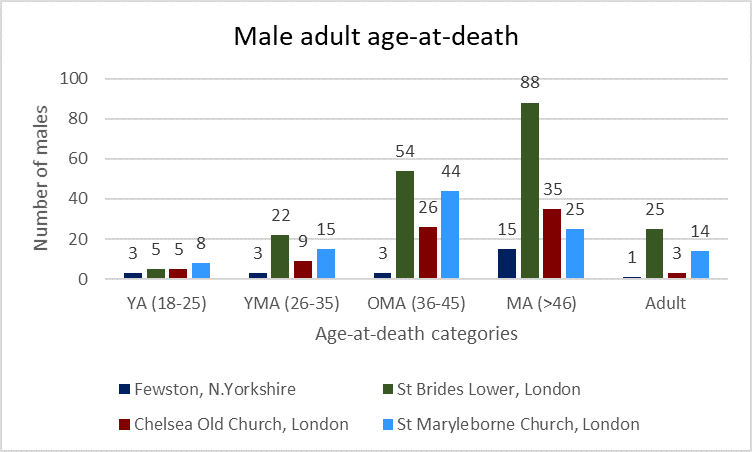
In the cemeteries assessed, age at death within adults appears regular, with the main peak of death occurring during later on in life, which was consistent between both sexes (Figure 10 and 11).
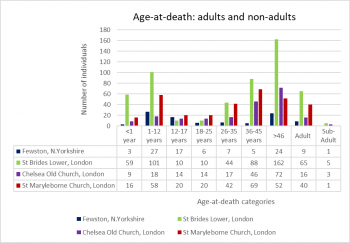
Sub-adult mortality was notably high for both lower and higher social classes (Figure 12); with the lower class prevalence calculating that 91.4% (160/175) of the children had died before they had reached 12 years of age, and a similar 91.0% (101/111) from the high-status cemeteries; indicating that poor health can occur during the crucial stages of development for all social classes.
Infant mortality, however, was greater in poorer socioeconomic assemblage with 3.7% (59/175) of the infants dying before the age of 1. In contrast, the prevalence of infant mortality from the high-status cemeteries calculated to be 22.5% (25/111) (Figure 12). Therefore, although there are multiple factors for high infant mortality, it can be suggested that those from a poorer economic status were possibly more susceptible to fatality and disease from malnourished mothers, or conversely predisposed to other diseases from conditions such as rickets (Kirby 2013, 49; Gowland 2018, 158; Gowland et al 2018, 26).
Discussion
Rural versus Urban Environment
As Industrialisation lead to rapid migrations of families to major cities due to the increase in jobs and wages; this period of transition lead to a parallel increase in vulnerability to the exposure of new pathogens, particularly affecting those already susceptible or experiencing illness’ attributed to dietary deficiencies (Roberts and Cox 2003, 299).
Therefore to an extent individuals who lived in major trading urban centres such London, were less likely to maintain sound health and diet due to the pollution. However, the lower classes were at a greater risk, as a result of the issues that arise with overcrowding and subsequent poor sanitation (Mays et al. 2008, 87).
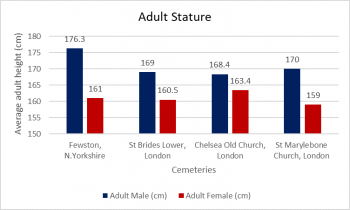
Furthermore, an important factor that affected the health of both social classes was the regional accessibility to food, in addition to the cost of fuel. Roberts and Cox (2003, 308) noted that socioeconomic status can often be translated into stature, however for many post-medieval individuals, arguably, the type of environment inhabited would have been more of an influential factor than status alone. For instance, significant use of fresh milk was suggested to have been nearly absent in southern and eastern English counties; or certainly largely adulterated by the time that milk had reached the consumer (Horrell and Oxley 2012b, 17; Roberts and Cox 2003, 310).
On the whole, individuals from a rural background were more likely to prepare home-baked foods than purchase shop-bought food which contained chemical traces, which would have had adverse effects on nutrition and health for all social classes (Gowland et al. 2018, 23; Roberts and Manchester 2010, 21; Roberts and Cox 2003, 312).
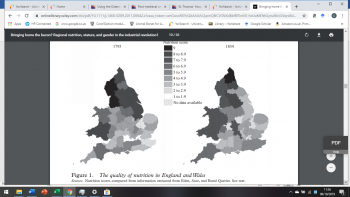
As seen in Figure 13, the regional nutritional values demonstrate vast variability between neighbouring counties; which supports the positive correlation in figure 14 between adult stature and regionality. Noticeably, the average height (cm) for adult males in London remained within a 2cm bracket, which is a stark contrast to males from urban north Yorkshire who were at least 6.3cm taller than their urban counterparts.
Age and survivability
To an extent, it is expected that adults are more likely to display evidence of poor health, due to longer exposure to disease and possible hazards, in addition to the overall disadvantages of ageing on male and female bones (Willson et al. 2015, 65; Weaver 1998, 39). However, an important point that has yet to be discussed is the impact of work-related trauma on the remains of lower-class children who were forced into labour. Factories and mills would have been highly hazardous work places, and working in such environments would have increased the risk of accidental fractures, or amputations, as a result of smaller children operating heavy machinery (Gowland 2018, 153).
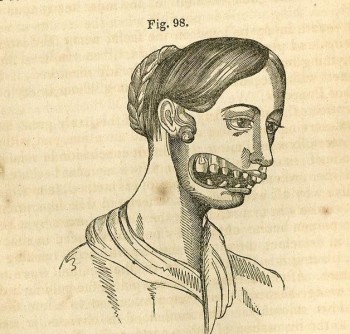
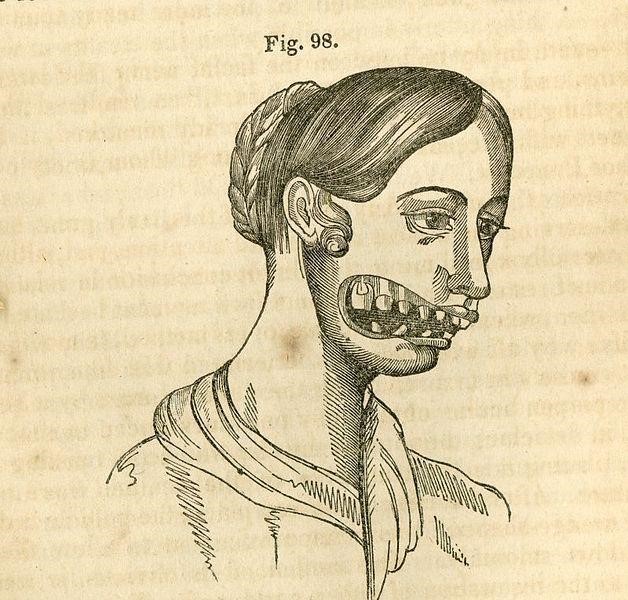
Fractures and amputations were not the only types of injuries sustained in this working environment; over-exposure to toxic chemicals has been shown to have caused respiratory-induced trauma in some non-adults from other poor-status cemeteries. An extreme case of respiratory-induced trauma was discovered on the remains of a 12-14-year-old from Coach Lane cemetery near Newcastle (Figure 15). Osteologists concluded that this was an example of over-exposure to phosphorous fumes from creating strike-anywhere matches in poorly ventilated factories (Roberts et al. 2016, 44). This type of work was noted to have attracted only “the poorest labourers”, with the condition itself creating necrosis of the jaw, which would have been highly stigmatised due to the odour (Gowland 2018, 150).
Conclusion
It can be argued that social status was a substantial influential factor in determining the diet, and subsequent health, of post-medieval adults and non-adults. However, it was not the catalyst for poor health as a whole. Arguably, the impact of urbanisation and industrialisation would have been detrimental for all social classes who lived and worked in an overpopulated urban centre. Arguably, the risk of lower-class individuals from urban cities was greater. This is based largely on the lack of nutrition and dire living and working conditions in which poorer families endured daily. A contemporary writer observed that even the most skilled labourers were “constantly exposed to loss of food”, which consequently resulted in “death by starvation” (Engels 2009, 85). This can be confirmed skeletally by the presence of conditions aforementioned, however it is worth considering the number of individuals who may have died before skeletal manifestations took place (Wood et al. 1992, 345).
In conclusion, the impact of poverty and socio-economic status negatively influenced the health and diet of individuals across England. However, there was a slight regional bias to the extent of food and nutrition accessibility which would have played a part in maintaining health. Health and diet were thus, to an extent, governed by regionalism more specifically relating to the cost of fuel to prepare food, raw resources, and the quantity of common land available.
Appendix I: Prevalence References
|
Cemetery |
Sub-adults CPR% (n/N) |
Adults CPR% (n/N) |
Total Scurvy CPR% (n/N)
|
Reference |
|
Fewston, N.Yorkshire |
38.4% (15/39) |
0.0% (0/104) |
10.5% (15/143) |
Gowland et al 2018; Caffell and Holst 2010 |
|
St Brides Lower, London |
6.9% (12/175)
|
0.0% (0/369) |
7.8% (12/544 |
WORD Database Museum of London, 2019 |
|
Chelsea Old Church, London |
6.06% (2/33) |
0.0% (0/168)
|
2.0% (2/201) |
WORD Database Museum of London, 2019 |
|
St Marylebone Church, London |
6.4% (5/78)
|
0.0% (0/223) |
1.7% (5/301) |
WORD Database Museum of London, 2019 |
|
Cemetery |
Sub-adults CPR% (n/N) |
Adults CPR% (n/N) |
Total Rickets CPR% (n/N)
|
Reference |
|
Fewston, N.Yorkshire |
44.8% (13/29) |
0.0% (0/104) |
9.8% (13/133) |
Gowland et al 2018; Caffell and Holst 2010 |
|
St Brides Lower, London |
14.87% (26/175) |
0.0% (0/104) |
6.4% (35/544) |
WORD Database Museum of London, 2019 |
|
Chelsea Old Church, London |
12.1% (4/33) |
6.0% (10/168) |
7.0% (14/201) |
WORD Database Museum of London, 2019 |
|
St Marylebone Church, London |
27.0% (21/78) |
4.0% (9/223) |
10.0% (30/301) |
WORD Database Museum of London, 2019 |
|
Cemetery |
Sub-adults CPR% (n/N) |
Adults CPR% (n/N) |
Total DISH CPR% (n/N)
|
Reference |
|
Fewston, N.Yorkshire |
0.0% (0/50) |
0.0% (0/104) |
0.0% (0/154) |
Gowland et al 2018; Caffell and Holst 2010 |
|
St Brides Lower, London |
0.0% (0/175) |
2.4% (9/369) |
1.7% (9/544) |
WORD Database Museum of London, 2019 |
|
Chelsea Old Church, London |
0.0% (0/33) |
6.5% (11/168) |
5.5% (11/201) |
WORD Database Museum of London, 2019 |
|
St Marylebone Church, London |
0.0% (0/78) |
2.7% (6/223) |
2.0% (6/301) |
WORD Database Museum of London, 2019 |
|
Cemetery |
Sub-adults CPR% (n/N) |
Adults CPR% (n/N) |
Total GOUT CPR% (n/N)
|
Reference |
|
Fewston, N.Yorkshire |
0.0% (0/50) |
0.0% (0/104) |
0.0% (0/154) |
Gowland et al 2018; Caffell and Holst 2010 |
|
St Brides Lower, London |
0.0% (0/175) |
1.6% (6/369) |
1.1% (6/544) |
WORD Database Museum of London, 2019 |
|
Chelsea Old Church, London |
0.0% (0/33) |
2.4% (4/168) |
2.0% (4/201) |
WORD Database Museum of London, 2019 |
|
St Marylebone Church, London |
0.0% (0/78) |
0.9% (2/223) |
0.7% (2/301) |
WORD Database Museum of London, 2019 |
|
Cemetery |
Age-at-death reference |
|
Fewston, N.Yorkshire |
Gowland et al 2018; Caffell and Holst 2010 |
|
St Brides Lower, London |
WORD Database Museum of London, 2019 |
|
Chelsea Old Church, London |
WORD Database Museum of London, 2019 |
|
St Marylebone Church, London |
WORD Database Museum of London, 2019 |





{kind=link}
{kind=link}
{kind=link}