1. Introduction
Roman invasion and settlement of Britain (c. 41 – 410 AD) introduced a wave of urbanisation and subsequent regionally centralised areas of administration and authority. After the Iron Age, Roman influence resulted in a noticeable distinction in living standards in different settlements, which had a profound effect on the overall health of respective populations, evident from the categorised markers detected in contemporary palaeopathological studies of human remains. Skeletal health is considerably informative, providing data associated with intra-population mortality and morbidity rates, and how they were affected by agents such as diet, status, labour/inactivity, and exposure to the inhabited environments. The Roman author Varro distinguished two standard ways of living: urban and rural; he considered the rustic lifestyles of rural areas to be superior in morals and health, while wealth prospered more within towns and cities (Varro 1934, cited in Redfern et al., 2015). Varro’s point about health is fairly generalised. However, palaeopathological analysis of Romano-British human remains has recently provided further insight into the accuracy of this assertion, with recent studies providing comparative analyses of skeletal and dental pathology specific to the differences between various urban and rural sites in Roman Britain (Pitts and Griffin, 2012; Redfern et al., 2015, Griffin 2017). This study therefore aims to challenge the notion posed by those such as Varro, that there is an apparent dichotomy of settlement health characteristics, by observing collective portions of various pathology prevalence rates in urban and rural areas, and discussing the potential reasons for their presence. Identification of pathologies and their prevalence in the sites analysed will either reject or reinforce the perspective of set health differences between Roman settlements. Analysis predominantly focuses on Dorset’s Poundbury Camp, and its surrounding urban and rural sites, as well as York’s Hungate burial ground for further regional comparison.
1.1 Life, Death and Disease: Stressors of Health
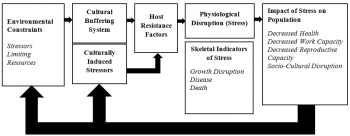
Before observing research findings of population pathology, the denotation of health and how its versatility can be affected must be considered. Health begins in utero and ends with death. It is fundamentally influenced by a variety of stressors, which can affect the skeletal system in different, albeit interlinking ways (Temple and Goodman, 2014). Such stresses include mechanical, nutritional, and disease-induced. They are also multi-faceted when concerning age, childhood experiences can have long-term developmentary implications on the physiological and psychological health of an individual as they grow into an adult, particularly concerning nutrition (Millet et al., 2011; Brickley, 2018). The aetiology of different pathological lesions that present themselves on the skeleton are rooted in these stressors; Goodman et al. (1984) and Goodman and Armelagos (revised, 1989) have attempted to structure the interpretation of these stress indicators in a paleoepidemiological model (see figure 1; Temple and Goodman, 2014: 187-188). This revised diagram demonstrates the separation of the skeletal indicators, namely (1) the manifestation of stress from (2) cause of functional loss. This distinction attempts to prevent ambiguity or further interpretative error.
2. Settlement Typologies
Among urban and rural sites are a variety of sub-categorised settlement types, either introduced during Romanisation of Britain or developed within existing Iron Age sites. These include hamlets, farmsteads, large towns, small towns, villages, and villas (Roberts and Cox, 2003). An analysis of settlement traits is touched upon in the next section to illustrate the different conditions to which their inhabitants were subjected, which ultimately affects aetiologies of disease and their prevalence.
2.1 Routes of Romano-British Rurality
Elements of both rural and urban life are key in explaining health exhibited by osteological signatures. After the Roman conquest, a predominantly rural Britain was significantly influenced in the formation and maintenance of new and its existing settlements. They were subject to the imposition of imperial appropriation (adapting to Roman social, economic and political standards), the introduction of new technologies and crops to improve productivity, and further expansion into the wider landscape; this was fundamentally coupled with an increase in population size through further contact with the Roman Empire and its continental sovereign states, and a rise in settlement density (van der Veen et al., 2008; Redfern et al., 2015). Rural settlements primarily included farmsteads, villages and villas; the latter was maintained by the poorer populace for high-status individuals (e.g Caerwent’s Silurum). Poorer settlements often rejected the introduction of Roman rectangular structures and exhibited an Iron Age continuance of roundhouse use and cohabitatation with animals (Roberts and Cox, 2003)., The Iron Age populations in the South and East of Britain evidently adopted and constructed large-scale mill corn dryers, granaries, and larger barns, resulting in an intensification of agricultural practice, potentially to meet the new demands of urban centres and military occupants (Taylor, 2001).
2.2 Urbanisation
Urbanisation following the Roman Conquest was a significant transition, rapidly increasing the number of small and large towns. These varied in size, density and housing type, and were incorporated into the Roman system of structured/ranked settlements, with the lowest classified as (1) Civitas: administrative and political centres with non-Roman citizen status; (2) Municipia, denoting allies of Rome; and (3) Colonia, for people with Roman citizenship (for example, Colchester, Gloucester, York, London and Lincoln) (Millet, 2001; Roberts and Cox, 2003; Redfern et al., 2015). The latter two types had specific forms in the landscape, typically possessing surrounding walls, orthogonal streets, small-scale horticulture, and sub-urban cemeteries along roads (Redfern et al., 2015). They essentially served as regional administrative, social, and economic hubs (Millet, 2001). The establishment of such areas may have indicated a native desire to follow a Roman way of life, and this urban transition drew people from across Britain and the continent alike (Millet, 2001). However, migration to these urban areas would have exposed individuals to diseases that had not been previously encountered or were rare, particularly due to increased population density as well as the cohabitation with animals. Roman York, for example, has yielded remains of grain weevils, rats, mice, fleas, lice, and intestinal parasites within past living spaces (Roberts and Cox, 2003). However, in comparison to rural areas, urban settings facilitated better access to sanitation, such as bathhouses and drainage/sewage systems from latrines, suggesting that urban health was well-regarded (Roberts and Cox, 2003). Urban environments thus developed some benefits with the introduction of better sanitation, although its compact conditions, sharing of living space, and welcoming of migrants, local and non-local to Britain, brought a range of new threats detrimental to the settlement population’s/inhabitants health and co-existence These could subsequently spread to the rural populations.
3. Skeletal and Dental Pathologies: A Comparative Analysis
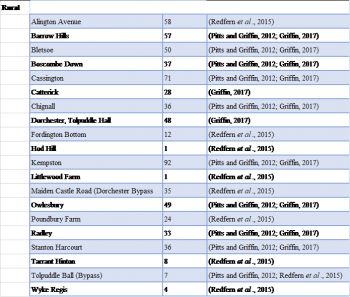
This analysis predominantly focuses on the studies of the intra-site variations in prevalence and frequency of pathological conditions, derived from individual site reports on human remains (Pitts and Griffin, 2012; Redfern et al., 2015; Griffin, 2017; see Tab. 1-3: 256-260; Tab. 1 & 4-5: 111 & 114-115; Tab. 1-2: 349 & 353, respectively). Approaches to the site comparisons analysed in these studies also differed, providing further variation between prevalence rates when considered together; Redfern et al., (2015) focused on a singular region’s variation (Dorset), while Pitts and Griffin (2012) and Griffin (2017) are considerably holistic with multiple regions used for comparison, including much of central, eastern and southern Britain (see tab. 1). Analysis of pathological conditions in Hungate, York, was also considered for an additional comparison between a provincial colonaie in the north, and its southern counterparts.

3.1 Methodological Limitations
Redfern et al’s (2015) partial data that excluded Poundbury from analysis to prevent statistical deviation in prevalence of pathological markers was disregarded as it is not a relevant covariate in this investigation. Likewise, nucleated/intermediate sites were also excluded to avoid complicating what have been regarded as characteristically rural and urban settlements. Studies also exhibit a lack of consistency in the types of pathological markers illustrated, limiting the overall intra-study comparison of prevalence rates, however, we can still see what is present from the individual studies and interpret the results within respective populations.
4. Results
4.1 Case Study: Pitts and Griffin, 2012
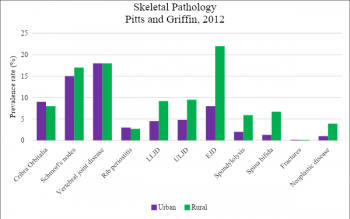
Resulting pathological prevalence rates from this study (see Fig. 2 and 3) are based on 20 burial sites (Urban: n = 10, Rural: n =10). Cribra orbitalia was not highly prevalent among the sites analysed, with no statistical significance between urban and rural settlements (p = 0.754), albeit slightly more prevalent in urban sites. oint disease was considerably prevalent in rural areas relative to urban areas; particularly concerning lower limb, upper limb, and extraverterbral joint disease. The crude prevalence rate of Schmorl’s nodes were similarly prevalent in urban and rural sites (Crude Prevalence Rate: 15% and 17% respectively), and vertebral joint disease was equally prevalent (18%). Rib periostitis and presence of fracture (<5%s were also similarly prevalent in both settings (<5%). Congenital diseases spondylolysis and spina bifida are both more prevalent in rural contexts; significantly higher than their presence in the urban sites (p = 0.025 and 0.028 respectively). Neoplastic disease prevalence was also significantly higher in rural settings (p = 0.051).
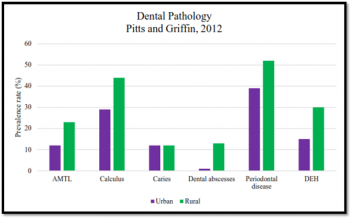
Dental pathology demonstrates a considerably higher prevalence across almost all categories among the rural sites analysed: Antemortem Tooth Loss (AMTL) (p = 0.014), dental abscesses (p = 0.002) periodontal disease (p = 0.041) and Dental Enamel Hypoplasia(DEH) (p = 0.030). Calculus was still relatively higher in prevalence in rural areas, though not statistically significant. Caries were an exception, which were equally prevalent (12%)
4.2 Case Study: Redfern et al., 2015
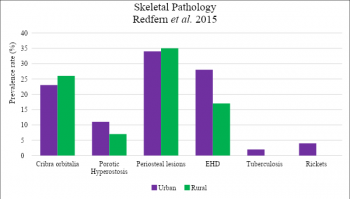
Redfern et al’s (2015) osteological analysis of pathologies (Fig. 4 and 5) is limited in its prevalence rates of metabolic and infectious diseases. This study analysed the differences between 9 rural and 10 urban sites within Dorset: the urban sites predominantly within or close to Dorchester. Metabolic diseases cribra orbitalia and porotic hyperostosis were varied, with a higher prevalence of the former in rural sites (26% vs. 23%) and the latter in urban sites (11% vs. 7%). . Periosteal lesions were highly prevalent in both urban and rural sites (34% and 35% respectively). Rickets and tuberculosis were only found on urban sites, and with low prevalence: 4% and 2% respectively.

Redfern et al.’s (2015) analysis of dental pathology, on the other hand, provided results contentious with that of Pitts and Griffin (2012) on the prevalence of caries and calculus; the most common of dental conditions. In this case, the urban sites exhibited a significantly higher prevalence of caries (55% vs. 35%; p = 0.002), and, though not statistically significant, also showed a higher prevalence of calculus (70% vs. 59%).
4.3 Case Study: Griffin, 2017
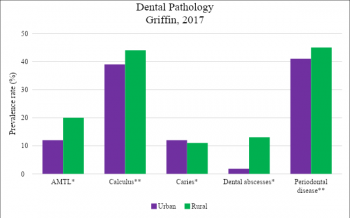
Griffin predominantly focused on the dental health (see fig. 6) of the chosen populations, exhibiting a similar correlation to Pitts and Griffin (2012) in the prevalence rates, albeit encompassing more sites (urban: n = 14, rural: n = 11). AMTL, calculus, dental abscesses and periodontal disease were more prevalent in rural sites than urban sites, with significantly higher dental abscesses (p = 0.003). Caries however were more prevalent in the urban populations, though marginally (12% vs. 11% respectively).
4.4 Case Study: Gomez, 2017: Hungate, York
Gomez’s (2017) study is small compared to the prior macroscopic analyses, providing a pathological examination (see Fig. 7 and 8) of 47 individual human remains in total, composed of 21 females and 26 males. Hungate is an urban district of York. However, as opposed to the other analyses there is a considerable prevalence of pathological conditions, although , this could be influenced by the small sample size and absence of data from other sites affecting the overall deviation. Comparisons to the other studies would also not be as representative in prevalence differences due to the disproportionate sample sizes. Nonetheless, the skeletal pathology of degenerative joint changes (DJC) appear to be the most prevalent (alongside PNBF: periosteal new bone formation) among the individuals (46.8%), opposing most correlations of rural-predominant joint disease found in Pitts and Griffin (2012), with exceptions to Schmorl’s nodes and general vertebral joint disease. The infectious disease sinusitis, like tuberculosis, is also present among the urban assemblage. Other conditions will be explained more in the discussion as they are not comparable with the other studies.
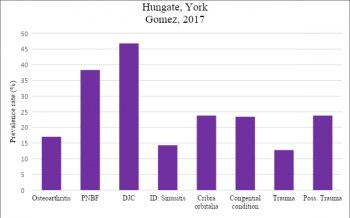
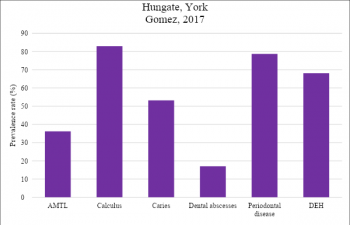
Calculus, caries, periodontal disease, and dental enamel hypoplasia are considerably prevalent at this site (ranging 53.2% - 83%), correlating with patterns exhibited by the Dorset populations (Redfern et al., 2015). AMTL and dental abscesses are similar in their lowest prevalence across each study.
5. Discussion
5.1 Skeletal Health: Pathologies
5.1.1 An Active Lifestyle: Movement and Age Progression
Intensity of labour or activities subject the body to wear and tear as we age, dependent on the rate and level at which this occurs. Joint diseases can be fundamental in informing us of this. They are associated with the spine, for example, and are typically mechanically induced, and developed through long-term stressors applied to the skeleton. For instance; heavy-loading activities for both males and females lead to vertebral conditions such as Schmorl’s nodes and spondylolysis, which are prevalent among both Romano-British urban and rural sites (Roberts and Manchester, 2012). Gradual ageing, in addition , is an equally relevant factor. However, , mechanical loading is more intense, and is a dynamic factor that exacerbates issues in the skeletal microstructures at a faster rate relative to the static nature of general ageing. Although, these two conditions in particular are ambiguous to some extent, and are thought to be the consequence of a combined congenital and developmental aetiology (Roberts and Manchester, 2012). Nevertheless, the results shown in figure 2 indicate that rural areas were more likely to exhibit these conditions (Pitts and Griffin, 2012). However, magnification of individual site analysis provides more insight on these generalised prevalence rates. Of Alington Avenue (rural Dorset) and West Tenter Street (WTS), London (urban), 16/109 individuals (CPR: 14.7%) of Alington Avenue, and 45/112 individuals (CPR: 40.2%) from WTS, were affected by spinal joint disease, showing an inverse of the results garnered by Pitts and Griffin (Robert and Cox, 2003). Likewise, Schmorl’s nodes also appeared less prevalent in Alington Avenue (CPR: 0.9%), while WTS exhibited a CPR of 23.6%, suggesting a higher prevalence of mechanical stress in the urban rather than rural areas (Roberts and Cox, 2003). There are posited reasons for the development of these pathological markers in urban and rural populous’; like certain civilian occupations common to both areas: building, horticulture, metalworking, textiles/fulling, leather-making, pottery, and facilitators of food and drink: butchers, bakers and fishmongers (Roberts and Cox, 2003). Agriculture was undertaken in some urban areas, although it was a more common practice in rural spaces due to the open landscape. Particularly since agriculture intensified, the production rate would have subsequently affected and increased the prevalence rate of such pathologies. Urban spaces tended to cater to gold, silver, and copper smithing, ironmaking, brick and tile production, glassmaking, and providing quarry constituents: stone, chalk, clay, gravel and flint (Roberts and Cox, 2003). Therefore, with a variety of work conducted in both areas one may see why there is an overlap between the prevalence rates; it is different work, but with similar mechanical requirements.
Furthermore, trauma of skeletal elements is also a consequence of mechanical stress or inflicted damage. Fractures, for instance, are the result of acute injuries, underlying disease that affects the integrity of the bone, and endurance of repeated mechanical stress (Roberts and Manchester, 2012). The results indicate that, among these populations, relative prevalence of trauma in both urban and rural populations was considerably rare. However, Hungate did exhibit trauma (12.8%) and possible trauma (23.8%), without specifically mentioning fractures. Molleson (1993: 199,citedin Hearne and Birbeck, 1999) argued that prevalence of fractures was higher in males due their involvement in physical activities such as construction, ploughing, and fighting. This would explain fractures caused by agricultural activity, and likely building in both urban and rural areas. The cohort of headless Romans found in York illustrate potentially different purposes as to how trauma was inflicted in urban environments. Müldner et al.’s (2011) study was of individuals, potentially slaves, gladiators or condemned noblemen, suggesting reasons other than work for trauma, like entertainment: gladiator fighting, or administering of punishment, within the urban context.
5.1.2 Provenancing Congenital Diseases
Congenital diseases and predispositions are predominantly influenced by genetics (90%), while only a small percentage (10%) is due to environmental factors. These environmental factors potentially include viral infections or nutritional deficiencies experienced by the mother, and passed to their offspring. Other speculation may consider the effects of herbal remedies used in Antiquity (Roberts and Manchester, 2012). The cause of congenital diseases is thus predominantly speculative in palaeopathological studies. Micro-analyses present very little evidence of their prevalence, though the Hungate population Gomez (2017) exhibited an unexpected prevalence of congenital disease among the female population (47.6%) as opposed to 3.8% of males.
5.1.3 Infectious Disease
Urbanisation’s characteristic increased and denser population would likely heighten the prevalence of infectious diseases due to the close proximity of humans and animals. Evidence of black rats, fleas, and human lice have been found in Roman York (Roberts & Cox, 2003). In addition, living within a polluted environment (burning fuel and living with animals) will have only exacerbated susceptibility to disease and increased the likelihood of contagion (Roberts and Cox, 2003). As tuberculosis can be contracted via the lungs from other humans or animals or the intestinal tract (from infected meat and milk); urban populations provided the perfect environment to promote such a disease (Roberts and Cox, 2003). This evidence would suffice to explain the small number of tuberculosis recordings from urban areas, while no such recordings are known from rural areas (Redfern et al., 2015).
5.2 Metabolic Diseases: Economy and Environment
5.2.1 Dental Pathology
Pitts and Griffin (2012) found that there was a higher prevalence of dental enamel hypoplasia in rural sites, a dental pathology that has been posited to indicate growth disruption (child-to-adolescence), caused by a number of speculated factors, including nutritional stress, genetics, localised trauma or chronic illnesses (Roberts and Manchester, 2012). It has also been compared to the way Harris Lines present in bones, which also show intermittent disruption in growth(Roberts and Manchester, 2012). This poor nutrition during the formative years has been credited to the urbanisation phase, which demanded rural surpluses of food to feed larger non-rural communities or military personnel, even though these rural sites relied on agriculturefor sustenance (Pitts and Griffin, 2012). This dependency on a agriculture would mean consumption of carbohydrate-based diets rich with high cereal content due to a lower availability of meat, increasing the prevalence rate of calculus and carious lesions, and subsequently contribute to, alongside poor oral hygiene, dental abscesses, periodontal disease, and antemortem tooth loss (Robert and Manchester, 2012; Griffin, 2017). This is evidence of an environmental constraint as stated by Temple and Goodman (2014) that denotes the stresses imposed by socio-political implementation rather than actual availability. Urban populations had greater access to meat and to other food groups (through trade), which prevents the occurrence of dental caries (Griffin, 2017). However, urban settlements have also been found to have a high dependency on a carbohydrate-based diet, resulting in a higher prevalence of carious lesions and dental calculus than would have been estimated, as found in the analysis of Dorset’s settlements (Redfern et al., 2015). Fruit and cooked starchy carbohydrates within the diet will also have contributed to these varied prevalence rates in urban and rural areas, and additionally, maintaining oral hygiene will likely have been easier in urban areas due to access to practitioners, which was likely limited in rural areas (Griffin, 2017).
5.2.2 Skeletal Pathology
Skeletal metabolic diseases such as cribra orbitalia and porotic hyperostosis are analogous with dental enamel hypoplasia and have been related to evidence of anaemia (iron deficiency) due to a lack of dietary constituents (Robert and Manchester, 2012). Rural and urban sites, again, yield non-indicative results other than that individuals suffered from nutrient deprivation, with Pitts and Griffin (2012) demonstrating that urban areas have a higher prevalence of cribra orbitalia, and Redfern et al. (2015) showing the inverse. Perhaps it is the inclusion of middle and eastern Romano-British sites that influence the balance of this prevalence, indicating that urban areas in mid-east Britain and rural Dorset possessed poorer nutrition than urban Dorset. The reason for the higher prevalence of CO in southern rural areas may derive from lack of dietary diversity resulting from comparably low access to other food groups gained elsewhere in urban areas through trade (Griffin, 2017).
Rickets, like tuberculosis, was only present on urban sites, although with a low prevalence rate (4%). The cause of Rickets is vitamin D deficiency; vitamin D is acquired through the absorption of calcium, phosphorus, and ultraviolet light by exposure to the sun (90% of vitamin D is acquired from sunlight, 10% from dietary sources) (Robert and Manchester, 2012). The presence on urban rather than agricultural sites may be due to social or occupational practice; agriculture is an outdoor activity , whereas urban populations may have worked or remained indoors more often, resulting in comparatively less exposure to the sun . Clothing and social culture may also have affected exposure of the skin to the sun (Roberts and Cox, 2003).
5.3 Study Limitations
There are various limitations in the approaches to analysing urban–rural differences in skeletal and dental health. Firstly, general sample sizes between rural and urban populations are inherently disproportionate due to a sparse versus dense settlement structure, although this can be considered as a variable that influences overall health. Additionally, site-specific sample sizes can be unwieldy due to variations among sites of the same category; deriving from preservation of skeletons and variation in settlement size; for instance Poundbury’s enormous human remains assemblage in comparison to other urban and rural sites . Intra-site variation is also too great and provides a generalisation of urban-rural differentiation, prompting the need for further magnification on site differences to accommodate and compliment macro-statistics. Griffin (2017) likewise suggests further work on a local level in order to understand the emerging palaeopathological patterns and their cause. Additional to this is the absent regard for intra-sex variation, looking wholly at settlements rather than whether there are specific influences on health between the sexes, as shown by the considerable variance between the Hungate male and females of York. Finally, while this essay is concerned with skeletal and dental health, mortality rates were disregarded because they are not exclusively contributory, as advised by Wood et al.’s (1992) osteological paradox: there are agents other than osteological markers that contribute to individual conditions, and thus subsequent mortality rates. However, it is acknowledged that a lower mortality rate would support the prospect of living longer, and thus a greater likelihood of developing various pathologies, like joint and metabolic diseases.
6. Conclusion
To conclude, there is differentiation in population health between rural and urban sites, though they are not set aside by definitive characteristics, evident by the inverse results and variation seen in the prevalence of pathologies across both site types. Pitts and Griffin (2012) and Griffin (2017) appear to concur that oral hygiene was worse among the rural settlements, while Redfern et al. (2015) contradicted that correlation. On the examination of skeletal health; joint disease seems to be the most explored, and possesses the highest prevalence among both urban and rural sites. There was an absence of comparable data from corresponding pathological conditions that limits the ability to see patterns in the statistics. Overall, the differences between rural and urban skeletal health are variable; similar conditions arise from activities or issues associated predominantly with respective settlements. The data does provide a breadth on skeletal and dental health in both urban and rural areas; the statistics coupled with historical narrative and archaeological material culture from such settlements allows us to provide reinforced speculation as to the reasons for resulting skeletal health across these sites (such as dietary access, work, leisure and administration). Recommended for future research is a localised analysis to further our understanding of health’s association with settlement type.